








 AR
AR 
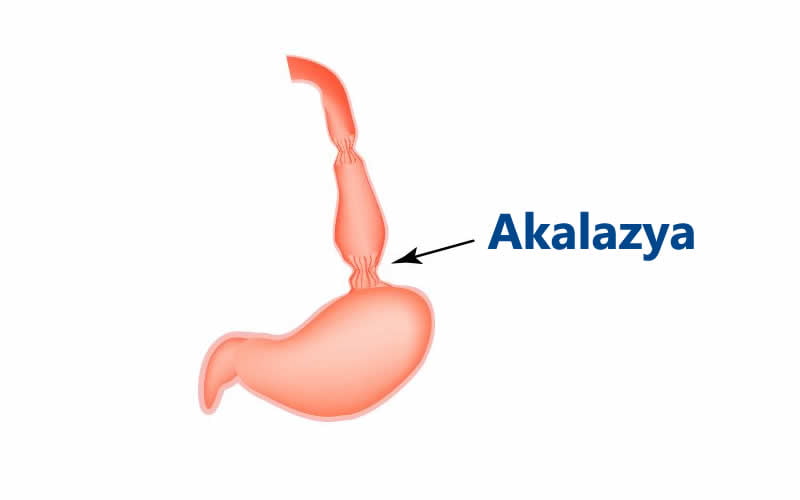
Achalasia is a rare disease that occurs due to impaired motility of the lower part of the esophagus. It is characterized by dysphagia, meaning difficulty in swallowing. Although it can be seen at any age, it is most common between the ages of 30 and 60, and it affects men and women equally.
Structure of the Esophagus

The esophagus consists of three layers. The outer layer is the longitudinal muscle layer, the inner layer is the circular muscle layer, and between them lies the myenteric plexus, which controls muscle activity. The innermost layer is the mucosa, which provides protection.
The esophagus connects the throat to the stomach and functions as a swallowing tube. In achalasia, the valve at the lower end of the esophagus fails to relax properly, preventing both solid and liquid foods from passing easily into the stomach.
How Does Achalasia Occur?
Achalasia develops due to dysfunction in the myenteric plexus. This leads to thickening of the muscles at the lower esophagus and stomach entrance, sometimes up to two or three times their normal size.
Normally, the lower esophageal valve opens for 5–10 seconds during swallowing to allow food passage. In achalasia, due to nerve damage and muscle thickening, food struggles to pass into the stomach and may accumulate in the esophagus.
What Do Patients Experience?
Patients often have difficulty eating. Many need to drink water to help swallow food and take longer to finish meals. They may also feel that they cannot reach a sense of fullness.
If such symptoms are present, medical evaluation should not be delayed.
Symptoms of Achalasia
Common symptoms include:
- Difficulty swallowing liquids despite being able to swallow solids initially
- Frequent respiratory infections
- Weight loss due to eating difficulties
- Food accumulation in the esophagus
- Regurgitation of food
- Bad breath
- Cough after meals
- Chest pain and burning sensation
How Is Achalasia Diagnosed?
Diagnosis can be challenging because symptoms may resemble reflux disease. In some cases, patients are mistakenly treated for reflux.
Definitive diagnosis methods include:
- Barium swallow test
- Gastroscopy
- Esophageal manometry
Achalasia Treatment
There is no definitive medical (drug) treatment for achalasia.
Treatment options include:
- Botox injection to relax lower esophageal muscles (temporary effect ~6 months)
- Balloon dilation to widen the narrowed area
Balloon dilation has an initial success rate of about 80%, but recurrence is common. There is also a small risk of esophageal rupture (~2%).
Surgical Treatment of Achalasia
Surgery aims to relieve symptoms and improve food passage. Two main surgical methods are used:
Heller Myotomy
Performed laparoscopically, this procedure involves cutting the thickened muscles. A fundoplication (using the upper part of the stomach) is often added to prevent reflux. It has a very high success rate when performed by experienced surgeons.
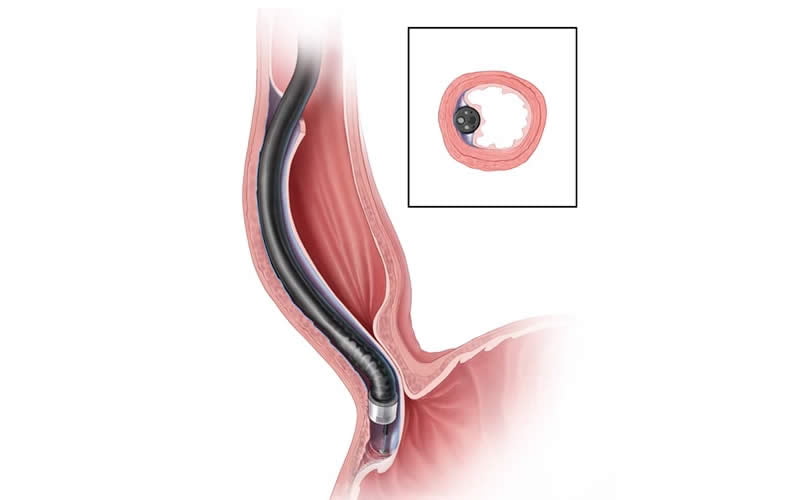
POEM (Per-Oral Endoscopic Myotomy)
This is an endoscopic technique where the muscle is cut from inside the esophagus. It is more expensive, and long-term success rates are still being evaluated.